Key Takeaways from the BC Dental Study Club Pediatric Dentistry Workshop
- Apr 16, 2025
- 6 min read

Hello Everyone!
I'm still buzzing from the absolutely fascinating pediatric dentistry workshop I attended with the BC Dental Study Club in Vancouver at the end of March 2025! My brain is packed with all sorts of insights, tips, and tricks for tackling those tiny, wiggly patients. The BC Dental Study Club did a fabulous job putting together this program! Forget your standard CE courses – this was a deep dive into the nitty-gritty, and I'm excited to share what I soaked up.
Educators:
The Grand Entrance (Waiting Room Intel!):
Apparently, the pediatric exam kicks off before they even grace your operatory chair! We learned to channel our inner Sherlock Holmes in the waiting room. Observing those parent-child dynamics, clocking the parents' anxiety levels (because, let's be real, their stress is totally contagious!), and even getting the lowdown from the front desk on those frequent flyer families – it's all intel for mentally prepping for the pint-sized patients heading your way.
Operation: First Look (The 30-Second Dash!):
A key takeaway? You often have a mere 30 seconds to get a decent peek inside a kiddo's mouth before the tiny jaws clamp shut like a well-oiled machine. So, prioritize! Forget leisurely perio charting for now. Scan for the big stuff, spot the obvious decay, and formulate your initial plan of attack – stat!
Risk Assessment: It's Not Just on Paper!
Understanding a child's caries risk? Apparently, it's the secret sauce for tailoring your treatment. Are we talking gentle fluoride varnish persuasion, or are we bracing ourselves for a GA scenario with a constellation of shiny new crowns? This risk assessment (think hygiene habits, past caries chronicles, family dental history) silently guides your decisions, even if you're not ticking off a checklist every single time.
X-Ray Escapades: Building Trust, One Click at a Time!
The wisdom shared was clear: exam before X-rays! You don't want to lose their precious cooperation before you've even had a proper look. And when it comes to those magical diagnostic images, the order matters: occlusals first ("cookie cracker" analogy – genius!), then bitewings once those back teeth start getting cozy around age three, and PAs for trauma or those sneaky deep lesions. And a word to the wise, fellow GPs: stick to intraoral bitewings for diagnosis! Treating based solely on panoramic bitewings for routine restorative work? Apparently, that's a no-go with the college. Also, recent X-rays are non-negotiable, even if GA is on the horizon.
Parental Maneuvering 101: Supportive Sideline Cheerleaders Only!
We gleaned some golden rules for navigating the parental landscape. Establish firm boundaries right from the get-go. They're there to offer moral support and maybe a hand squeeze, but absolutely no backseat dentistry or narrating the procedure! Let us wield our carefully curated, non-scary vocabulary.
The Pediatric Phrasebook: From Tooth Climbs to Tooth Showers!
Ditch the "rubber dam" and "high-speed handpiece"! We need a whole new dialect for our little patients. Think "tooth princess comb" for the explorer and "tooth soap" for your Etch. Get creative, rope in your assistants with the lingo – apparently, mermaid tales and superhero gadget analogies are fair game! Just remember to translate back to "adult speak" for the parents later. And pro-tip: weave a story into your explanations – it helps those amazing little imaginations visualize what's happening. Personalizing the language based on their interests (Spider-Man tools, anyone?) is also a win.
Treatment Tactics: Playing the Long Game (and Dodging GA Repeat Performances!):
Treatment planning in pediatrics is heavily influenced by factors like the patient's age and the strategic importance of the tooth (hello, exfoliation timelines!). It was pointed out that under GA, a more comprehensive approach is often favored to minimize the chances of needing another anesthetic down the road. That seemingly small occlusal pit could be hinting at something more extensive! So, when you refer for GA, give parents a heads-up that the pediatric dentist might discover more than initially meets the eye.
Minimally Invasive Marvels (and Knowing When to Pass):
We explored the realm of gentle dentistry, including:
ART/ITR (Atraumatic Restorative Treatment): Think of it as carefully scooping out the soft, mushy decay with a spoon excavator (gentle, gentle!) and then plugging the hole with glass ionomer or RMGI. Great for temporizing before a referral or in situations where traditional treatment isn't feasible. It’s all about caries control, not necessarily a picture-perfect restoration. Billing code? Apparently, 20111 for caries control.
Hall Crowns: Mind. Blown. No prep, no local – just cementing a stainless steel crown right over the decay using GI cement! Apparently, studies show surprisingly high success rates (think 90-95%) with success defined as no pain, no infection, or tooth loss before exfoliation. While the bite might initially open a tad, those little teeth have an amazing capacity to readjust. Separators can be your buddy for tight contacts.
Silver Diamine Fluoride (SDF): This stuff is like a superhero in a bottle (albeit one that turns decay black!). It arrests or slows down caries. For interproximal application, the super floss technique is key (Vaseline the face, dry angle, cotton roll – and gently wiggle that floss out!). Post-op? No eating/drinking for an hour and skipping flossing that night. Remember to give parents the choice, especially for anterior teeth, and explain the potential for black staining.
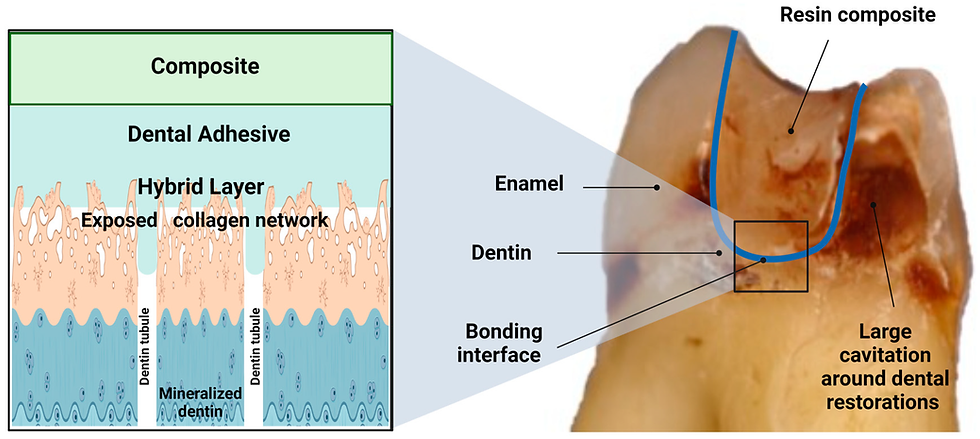
The Restorative Rodeo: Composites vs. Crowns (It's Not Always a Fair Fight!):
A sobering statistic: Class II composites in kiddos four and under have around a 50% failure rate. For those tiny patients with more extensive decay (more than a third into dentin), consider the crown!. And remember the mantra: a crown doesn't always mean a pulpotomy, but a pulpotomy definitely means a crown.
We even got into the nitty-gritty of stainless steel crown prep: flatten that occlusal surface, gently slide that interproximal bur through (imagine creating space!), and be strategic with buccal reduction. The crown should have that satisfying snap of retention, sit slightly subgingival, and not rock or rotate. Cementation is key, and don't forget to floss away the excess. For stubborn crowns, how pliers can be your friend for gentle removal.
Pulp Therapy Pointers (We Can Handle This!):
Pulpotomy is for vital teeth only! Access the pulp (occlusal reduction can help!), unroof that chamber (mind the tooth's unique anatomy – triangular in uppers, rectangular in lowers!). Clean gently with outward motions using a round bur, protecting that precious pulpal floor. Achieving hemostasis is the goal – various agents (ferric sulfate, MTA, saline) can be used. Remember, persistent bleeding might indicate lingering inflamed tissue. And that crown on top? Absolutely essential for long-term success. Avoid pulpectomies on those little incisors due to resorption concerns.
Referral Wisdom: Knowing Your Limits is Strength!
Knowing when to refer is as crucial as knowing how to treat. It’s a blend of your comfort level and the complexity of the case. When you do refer, educate parents on what to expect at the specialist. Document your recommendations thoroughly, even if initially declined.
Airway Awareness: The Buzz in Pediatrics:
Airway dentistry is definitely a hot topic. While the evidence is still evolving, it's important to be aware of signs like grinding, large tonsils, and mouth breathing. Assess, but be mindful of over-promising.
Antibiotic Allies (A Quick Cheat Sheet!):
For those little infections:
Less than 15 kg: Amoxicillin 125 mg/5ml, 5ml PO TID for 7-10 days.
15-30 kg: Amoxicillin 250 mg/5ml, 5ml PO TID for 7-10 days.
Parting Thoughts (and Maybe a Touch of Cement Dust!):
What a jam-packed and incredibly valuable weekend! From deciphering waiting room vibes to mastering the art of the stainless steel crown, this workshop offered a fantastic blend of theory and hands-on practice. The biggest takeaway? Pediatric dentistry has its own unique demands, requiring a special mindset, a playful vocabulary, and a whole lot of patience (for both the tiny patients and their grown-ups!).
So, the next time a little one hops into your chair, remember the 30-second scan, embrace the "tooth shower," and don't shy away from the mighty stainless steel crown. And when in doubt? Referral is always a wise option (and maybe a strong coffee afterwards!).
Keep those little smiles bright!
P.S. Huge thanks to the BC Dental Study Club for organizing such an insightful and practical course! And yes, there were definitely some great goodies to take home – always a bonus after a weekend of learning! 😉
For More Information:

Comments